www.TheCardiacICU.com
Форум посвящён вопросам кардиоанестезиологии, кардиохирургии, а также смежным дисциплинам. The forum is devoted to cardiac anesthesia, cardiac surgery and allied topics.
Лактатацидоз
Модератор: Евгений Хоменко
Сообщений: 3
• Страница 1 из 1
Лактатацидоз
![]() Валера » Пн авг 01, 2011 12:51 pm
Валера » Пн авг 01, 2011 12:51 pm
Вопрос по наболевшей теме - лактатацидоз. Периодически наблюдаем Лактат 20ммоль/л через 5-6 часов после отлучения от ИК. Отлучение обычное, без особых усилий (анестезиолог тоже не кричит караул, со слов - без особенных усилий). Пациенты разные от молодых с короткими ИК до тяжелых и ИК около 3часов. Откуда берется такой лактат?
- Валера
- Сообщения: 1
- Зарегистрирован: Пн авг 01, 2011 12:14 pm
![]() Alexey Dyachkov » Ср авг 03, 2011 3:15 am
Alexey Dyachkov » Ср авг 03, 2011 3:15 am
Факторы, судя по литературе такие: время ИК, степень гипотермии и гипергликемии, использование вазопрессоров.
Здесь я положил одну статью: Severe lactic acidosis after cardiac surgery: Sign of perfusion deficits?
Boldt, J., Piper, S., Murray, P., Lehmann, A. Correspondence address
Dept. Anesth. Intensive Care Med., Klinikum der Stadt Ludwigshafen, Bremserstr 79, D-67063 Ludwigshafen, Germany
http://www.zshare.net/download/93267250756b8a7d/
_________________________
И ещё пара абстрактов:
Critical Care
Volume 10, 2006, Article number R167
ISSN: 13648535
Hyperlactatemia during cardiopulmonary bypass: Determinants and impact on postoperative outcome
Ranucci, M.Email this author, De Toffol, B.Email this author, Isgrò, G.Email this author, Romitti, F.Email this author, Conti, D.Email this author, Vicentini, M.Email this author Correspondence address
Department of Cardiovascular Anesthesia and Intensive Care, IRCCS Policlinico S. Donato, Via Morandi 30, 20097 San Donato Milanese, Milan, Italy
Abstract
Introduction: Hyperlactatemia during cardiopulmonary bypass is relatively frequent and is associated with an increased postoperative morbidity. The aim of this study was to determine which perfusion-related factors may be responsible for hyperlactatemia, with specific respect to hemodilution and oxygen delivery, and to verify the clinical impact of hyperlactatemia during cardiopulmonary bypass in terms of postoperative morbidity and mortality rate. Methods: Five hundred consecutive patients undergoing cardiac surgery with cardiopulmonary bypass were admitted to this prospective observational study. During cardiopulmonary bypass, serial arterial blood gas analyses with blood lactate and glucose determinations were obtained. Hyperlactatemia was defined as a peak arterial blood lactate concentration exceeding 3 mmol/l. Pre- and intraoperative factors were tested for independent association with the peak arterial lactate concentration and hyperlactatemia. The postoperative outcome of patients with or without hyperlactatemia was compared. Results: Factors independ ently associated with hyperlactatemia were the preoperative serum creatinine value, the presence of active endocarditis, the cardiopulmonary bypass duration, the lowest oxygen delivery during cardiopulmonary bypass, and the peak blood glucose level. Once corrected for other explanatory variables, hyperlactatemia during cardiopulmonary bypass remained significantly associated with an increased morbidity, related mainly to a postoperative low cardiac output syndrome, but not to mortality. Conclusion: Hyperlactatemia during cardiopulmonary bypass appears to be related mainly to a condition of insufficient oxygen delivery (type A hyperlactatemia). During cardiopulmonary bypass, a careful coupling of pump flow and arterial oxygen content therefore seems mandatory to guarantee a sufficient oxygen supply to the peripheral tissues.
____________________________
Critical Care Medicine
Volume 25, Issue 1, January 1997, Pages 46-51
ISSN: 00903493
Type B lactic acidosis following cardiopulmonary bypass
Raper, R.F.a b , Cameron, G.a , Walker, D.a , Jane Bowey, C.a Correspondence address
a Cardiothoracic Intensive Therapy Unit, Royal North Shore Hospital, Sydney, NSW, Australia
b C/ITU, Royal North Shore Hospital, Pacific Highway, St. Leonards, NSW 2065, Australia
Abstract
Objective: To describe, characterize, and identify the associations of postcardiac surgical lactic acidosis occurring in the absence of clinical evidence of tissue hypoperfusion. Design: The preliminary study is a report of a series of observations in 12 patients. The prospective study is also observational, involving the structured collection of hemodynamic and metabolic variables in a prescribed series of patients. Setting: Cardiac surgical intensive care unit of a university teaching hospital. Patients: Twelve patients who developed an unexplained lactic acidosis after cardiac surgery are reported in the preliminary study. The prospective study involved observations in 112 consecutive patients undergoing cardiopulmonary bypass for cardiac surgery. Interventions: None. Measurements and Main Results: Preliminary study: Cardiac index was increased before, during and after recovery from lactic acidosis. Recovery from lactic acidosis was associated with a decrease in oxygen transport index and significant increases in oxygen consumption index and oxygen extraction ratio. Prospective study: Hemodynamic, oxygen transport, and oxygen consumption variables, together with arterial blood gas and lactate concentrations, were assessed every 6 hrs for 24 hrs after surgery. Sixteen patients developed lactic acidosis (peak lactate concentration >5.0 mmol/L). Compared with the remainder of the patients, this subgroup had longer duration of cardiopulmonary bypass (116 ± 31 vs. 76 ± 31 mins, p < .01), greater intraoperative hypothermia (24.9 ± 2.0° vs. 26.6 ± 2.3°C, p < .01), more frequent requirement for vasopressor agents (14/16 vs. 35/96, p < .05) and a higher frequency of hyperglycemia (15/16 vs. 28/96, p < .01). Hemodynamic variables, including cardiac index, were remarkably similar in the acidotic and nonacidotic groups. All of the acidotic patients, in both parts of this study, recovered from their acidosis. Eleven of the patients in the preliminary study and all of the 16 acidotic patients in the prospective study were ultimately discharged from the hospital. Conclusions: This report documents the occurrence of lactic acidosis in a subgroup of patients undergoing cardiopulmonary bypass. The pathogenesis of this disorder is uncertain, but it appears to not relate to inadequate oxygen delivery. Systemic vasodilation and reduced oxygen extraction appear to be features of this disorder, which has an excellent prognosis.
Здесь я положил одну статью: Severe lactic acidosis after cardiac surgery: Sign of perfusion deficits?
Boldt, J., Piper, S., Murray, P., Lehmann, A. Correspondence address
Dept. Anesth. Intensive Care Med., Klinikum der Stadt Ludwigshafen, Bremserstr 79, D-67063 Ludwigshafen, Germany
http://www.zshare.net/download/93267250756b8a7d/
_________________________
И ещё пара абстрактов:
Critical Care
Volume 10, 2006, Article number R167
ISSN: 13648535
Hyperlactatemia during cardiopulmonary bypass: Determinants and impact on postoperative outcome
Ranucci, M.Email this author, De Toffol, B.Email this author, Isgrò, G.Email this author, Romitti, F.Email this author, Conti, D.Email this author, Vicentini, M.Email this author Correspondence address
Department of Cardiovascular Anesthesia and Intensive Care, IRCCS Policlinico S. Donato, Via Morandi 30, 20097 San Donato Milanese, Milan, Italy
Abstract
Introduction: Hyperlactatemia during cardiopulmonary bypass is relatively frequent and is associated with an increased postoperative morbidity. The aim of this study was to determine which perfusion-related factors may be responsible for hyperlactatemia, with specific respect to hemodilution and oxygen delivery, and to verify the clinical impact of hyperlactatemia during cardiopulmonary bypass in terms of postoperative morbidity and mortality rate. Methods: Five hundred consecutive patients undergoing cardiac surgery with cardiopulmonary bypass were admitted to this prospective observational study. During cardiopulmonary bypass, serial arterial blood gas analyses with blood lactate and glucose determinations were obtained. Hyperlactatemia was defined as a peak arterial blood lactate concentration exceeding 3 mmol/l. Pre- and intraoperative factors were tested for independent association with the peak arterial lactate concentration and hyperlactatemia. The postoperative outcome of patients with or without hyperlactatemia was compared. Results: Factors independ ently associated with hyperlactatemia were the preoperative serum creatinine value, the presence of active endocarditis, the cardiopulmonary bypass duration, the lowest oxygen delivery during cardiopulmonary bypass, and the peak blood glucose level. Once corrected for other explanatory variables, hyperlactatemia during cardiopulmonary bypass remained significantly associated with an increased morbidity, related mainly to a postoperative low cardiac output syndrome, but not to mortality. Conclusion: Hyperlactatemia during cardiopulmonary bypass appears to be related mainly to a condition of insufficient oxygen delivery (type A hyperlactatemia). During cardiopulmonary bypass, a careful coupling of pump flow and arterial oxygen content therefore seems mandatory to guarantee a sufficient oxygen supply to the peripheral tissues.
____________________________
Critical Care Medicine
Volume 25, Issue 1, January 1997, Pages 46-51
ISSN: 00903493
Type B lactic acidosis following cardiopulmonary bypass
Raper, R.F.a b , Cameron, G.a , Walker, D.a , Jane Bowey, C.a Correspondence address
a Cardiothoracic Intensive Therapy Unit, Royal North Shore Hospital, Sydney, NSW, Australia
b C/ITU, Royal North Shore Hospital, Pacific Highway, St. Leonards, NSW 2065, Australia
Abstract
Objective: To describe, characterize, and identify the associations of postcardiac surgical lactic acidosis occurring in the absence of clinical evidence of tissue hypoperfusion. Design: The preliminary study is a report of a series of observations in 12 patients. The prospective study is also observational, involving the structured collection of hemodynamic and metabolic variables in a prescribed series of patients. Setting: Cardiac surgical intensive care unit of a university teaching hospital. Patients: Twelve patients who developed an unexplained lactic acidosis after cardiac surgery are reported in the preliminary study. The prospective study involved observations in 112 consecutive patients undergoing cardiopulmonary bypass for cardiac surgery. Interventions: None. Measurements and Main Results: Preliminary study: Cardiac index was increased before, during and after recovery from lactic acidosis. Recovery from lactic acidosis was associated with a decrease in oxygen transport index and significant increases in oxygen consumption index and oxygen extraction ratio. Prospective study: Hemodynamic, oxygen transport, and oxygen consumption variables, together with arterial blood gas and lactate concentrations, were assessed every 6 hrs for 24 hrs after surgery. Sixteen patients developed lactic acidosis (peak lactate concentration >5.0 mmol/L). Compared with the remainder of the patients, this subgroup had longer duration of cardiopulmonary bypass (116 ± 31 vs. 76 ± 31 mins, p < .01), greater intraoperative hypothermia (24.9 ± 2.0° vs. 26.6 ± 2.3°C, p < .01), more frequent requirement for vasopressor agents (14/16 vs. 35/96, p < .05) and a higher frequency of hyperglycemia (15/16 vs. 28/96, p < .01). Hemodynamic variables, including cardiac index, were remarkably similar in the acidotic and nonacidotic groups. All of the acidotic patients, in both parts of this study, recovered from their acidosis. Eleven of the patients in the preliminary study and all of the 16 acidotic patients in the prospective study were ultimately discharged from the hospital. Conclusions: This report documents the occurrence of lactic acidosis in a subgroup of patients undergoing cardiopulmonary bypass. The pathogenesis of this disorder is uncertain, but it appears to not relate to inadequate oxygen delivery. Systemic vasodilation and reduced oxygen extraction appear to be features of this disorder, which has an excellent prognosis.
-

Alexey Dyachkov - Site Admin
- Сообщения: 408
- Зарегистрирован: Вс май 14, 2006 7:43 pm
- Откуда: Geisinger Medical Center
![]() Евгений Хоменко » Чт авг 11, 2011 3:06 pm
Евгений Хоменко » Чт авг 11, 2011 3:06 pm
Я бы добавил к перечисленным Алексеем факторам провоцирующим или сопровождающим (как угодно) развитие лактатацидоза и гиперлактатемии без ацидоза :
- скорость согревания (чем быстрее, тем выше вероятность развития)
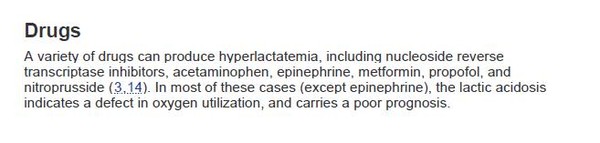
- помимо вазопрессоров, использование катехоламинов (бета-миметики), это известный фактор провокации продукции лактата в отделениях реанимации (вырезка из ICU book, 2007)
В целом сам по себе лактат особого вреда не несет, поэтому вопрос:
почему Вас это беспокоит?
что Вы предпринимаете в таких случаях (агрессивное лечение [бикарбонат, катехоламины, гемотрансфузия] или даете время на самоисцеление при условии, что нет крупного инфаркта и подтвержденного малого выброса)
- скорость согревания (чем быстрее, тем выше вероятность развития)
- помимо вазопрессоров, использование катехоламинов (бета-миметики), это известный фактор провокации продукции лактата в отделениях реанимации (вырезка из ICU book, 2007)
В целом сам по себе лактат особого вреда не несет, поэтому вопрос:
почему Вас это беспокоит?
что Вы предпринимаете в таких случаях (агрессивное лечение [бикарбонат, катехоламины, гемотрансфузия] или даете время на самоисцеление при условии, что нет крупного инфаркта и подтвержденного малого выброса)
MD
Leningrad Regional Clinical Hospital
Cardiac Anesthesia Division
Leningrad Regional Clinical Hospital
Cardiac Anesthesia Division
- Евгений Хоменко
- Site Admin
- Сообщения: 517
- Зарегистрирован: Пн май 15, 2006 12:30 pm
- Откуда: St. Petersburg
Сообщений: 3
• Страница 1 из 1
Вернуться в Дискуссии / Discussions
Кто сейчас на конференции
Сейчас этот форум просматривают: нет зарегистрированных пользователей и гости: 2